Summary / Overview
- Parvovirus B19 causes erythema infectiosum, a mild childhood exanthem characterized by the “slapped-cheek” rash.
- It infects erythroid precursor cells → temporary suppression of red-cell production, significant in hemolytic disorders.
- Usually self-limiting in children, but can cause aplastic crisis, fetal hydrops, or arthritis in adults.
Etiology
- Parvovirus B19 is a single-stranded DNA virus belonging to the Parvoviridae family.
- Transmission occurs via respiratory droplets, vertical (mother → fetus), and blood products.
- Virus has a strong tropism for erythroid progenitor cells in the bone marrow → transient red cell aplasia.
- Infectivity is highest *before* rash onset when viremia peaks.
Pathogenesis
- Parvovirus B19 targets erythroid precursor cells in the bone marrow via the P-antigen receptor.
- After respiratory entry → virus replicates in the nasopharynx → viremia develops.
- Mass destruction of erythroid precursors → transient arrest of erythropoiesis (RBC production stops for 7–10 days).
- Immune complex formation (virus + IgM) causes the characteristic “slapped-cheek” rash and arthralgia.
- During pregnancy → infection can cause fetal anemia → hydrops fetalis due to high-output cardiac failure.
Symptoms
- Bright red “slapped-cheek” rash
- Lacy (reticular) rash on arms and trunk
- Persistent anemia in immunocompromised
Signs
- Lacy, reticular rash on limbs and trunk
- No significant pharyngitis or conjunctivitis
Clinical Features
- Biphasic illness pattern
- Initial phase (non-specific):
- Rash phase:
- Arthropathy (common in adults):
- Hematologic features:
- Pregnancy-specific features:
- Immunocompromised hosts:
Investigations
- Diagnosis usually clinical during classic rash phase
- Serology:
- PCR for Parvovirus B19 DNA:
- CBC:
- Reticulocyte count:
- Ultrasound (in pregnancy):
- Bone marrow (rare):
Differential Diagnosis
- Rubella (German measles)
- Measles
- Roseola (HHV-6/7)
- Scarlet fever
- Dengue fever rash
- Drug-induced exanthem
- Systemic juvenile idiopathic arthritis (Still's disease)
- Lupus flare or viral-type malar rash
- Aplastic anemia of other causes
Complications
- Transient aplastic crisis (TAC)
- Chronic red-cell aplasia
- Hydrops fetalis (in pregnancy)
- Fetal loss or miscarriage
- Arthropathy
- Myocarditis
- Neurologic complications (rare)
- Hepatitis or hepatic dysfunction
- Vasculitic or purpuric eruptions
Treatment
- No specific antiviral therapy required in most cases
- Supportive care
- Arthropathy management
- IVIG for immunocompromised with chronic anemia
- Blood transfusion for severe anemia
- Fetal management during pregnancy
- Isolation not required once rash appears
- Avoid exposure during pregnancy (preventive advice)
Prevention
- No vaccine available
- Good hand hygiene reduces transmission
- Avoid close contact during the viremic phase
- Pregnancy precautions
- Infection control in schools & healthcare
- Protection of high-risk groups
- Environmental cleaning
Serotypes / Subtypes
- Only one major human pathogenic serotype (B19)
- Genotypes show minor molecular variation
- No clinically relevant subtype differences
- Stable virus with low antigenic drift
Pathology
- Selective tropism for erythroid precursor cells
- Transient red cell aplasia
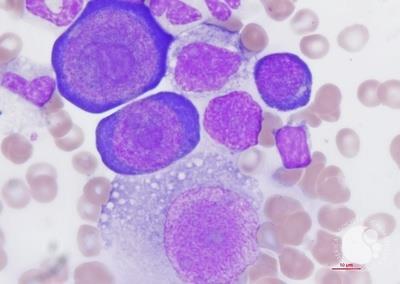
- Characteristic “giant pronormoblasts”
- Immune complex–mediated rash & arthralgia
Radiology / Imaging
- Usually normal chest radiograph in erythema infectiosum
- Key modality for detecting fetal complications
Notes / Teaching points
- Why does Parvovirus B19 cause sudden severe anemia?
- Why is transient aplastic crisis seen only in patients with chronic hemolytic anemias?
- Why does the classic “slapped-cheek rash” occur?
- Why do adults with B19 get arthralgia instead of rash?
- Why can Parvovirus B19 infect the fetus but not cause structural malformations?
- Why is fetal infection dangerous in the 2nd trimester?
- Why does Parvovirus not cause chronic hemolysis?
- Why are immunocompromised patients at risk for chronic infection?
- Why do some patients show only mild flu-like symptoms?
- Why doesn’t Parvovirus B19 commonly cause respiratory symptoms?
Biphasic illness pattern
1) Initial viremic phase
2) Immune-mediated rash/arthropathy phase
Initial phase (non-specific):
Mild fever
Headache
Myalgia
Malaise
Sore throat
Sometimes mild cough or rhinorrhea
Rash phase:
Slapped-cheek facial erythema
Lacy, reticular maculopapular rash on trunk and limbs
Rash may recur with heat, sunlight, exercise, or stress
Arthropathy (common in adults):
Symmetric pain and stiffness in small joints (hands, wrists)
Knees and ankles may be involved
Usually resolves in weeks
Hematologic features:
Transient aplastic crisis in patients with hemolytic disorders
Worsening anemia in pregnancy or immunocompromised patients
Pregnancy-specific features:
Risk of fetal hydrops due to severe fetal anemia
Possible fetal loss in early pregnancy
Immunocompromised hosts:
Prolonged anemia
Chronic infection with persistent viremia
Transient aplastic crisis (TAC)
Occurs in patients with increased red-cell turnover (sickle cell disease, thalassemia, hereditary spherocytosis). Sudden drop in Hb + reticulocytopenia.
Chronic red-cell aplasia
Seen in immunocompromised patients (HIV, transplant, leukemia). Persistent anemia due to inability to clear virus.
Hydrops fetalis (in pregnancy)
Maternal infection → fetal anemia → high-output cardiac failure → hydrops. Risk highest in 1st and 2nd trimester.
Fetal loss or miscarriage
If severe fetal anemia develops; usually between 17–24 weeks gestation.
Arthropathy
Immune-mediated symmetric small-joint pain/swelling; common in adult women; usually self-limited.
Myocarditis
Rare but reported; can cause arrhythmia or heart failure.
Neurologic complications (rare)
Encephalitis, meningitis, peripheral neuropathy—immune-mediated.
Hepatitis or hepatic dysfunction
Mild transient elevation of transaminases in some cases.
Vasculitic or purpuric eruptions
Including papular-purpuric glove-and-sock syndrome (PPGSS).
Rubella (German measles)
Postauricular lymphadenopathy, mild fever, faster-spreading rash; IgM/IgG serology differentiates.
Measles
High fever, cough–coryza–conjunctivitis, Koplik spots, confluent rash spreading cephalocaudally.
Roseola (HHV-6/7)
High fever for 3–4 days → fever suddenly resolves → rash appears afterward.
Scarlet fever
Sandpaper rash, strawberry tongue, Pastia lines; throat swab positive for Group A Streptococcus.
Dengue fever rash
Generalized erythematous rash or “islands of white in a sea of red”; thrombocytopenia and severe myalgia.
Drug-induced exanthem
History of new medication, pruritic morbilliform rash; no reticulocytopenia.
Systemic juvenile idiopathic arthritis (Still's disease)
Evanescent salmon-pink rash + fever spikes; arthritis prominent.
Lupus flare or viral-type malar rash
Photosensitive malar rash sparing nasolabial folds; ANA/anti-dsDNA assist diagnosis.
Aplastic anemia of other causes
Medication-induced, autoimmune, or bone-marrow failure syndromes; marrow study differentiates.
Parvovirus B19 is a single-stranded DNA virus belonging to the Parvoviridae family.
Transmission occurs via respiratory droplets, vertical (mother → fetus), and blood products.
Virus has a strong tropism for erythroid progenitor cells in the bone marrow → transient red cell aplasia.
Infectivity is highest *before* rash onset when viremia peaks.
Diagnosis usually clinical during classic rash phase
Serology:
IgM antibodies → indicates recent infection
IgG antibodies → indicates past infection or immunity
Useful in pregnancy, atypical cases, or immunocompromised patients
PCR for Parvovirus B19 DNA:
Highly sensitive
Detects viremia
Indicated in: pregnancy, aplastic crisis, immunocompromised patients, ambiguous serology
CBC:
Mild anemia
Reticulocytopenia (important clue)
Possible neutropenia or thrombocytopenia in some cases
Reticulocyte count:
Low retic count confirms temporary marrow suppression
Ultrasound (in pregnancy):
Evaluate fetus for hydrops fetalis
Look for ascites, skin edema, pleural/pericardial effusion, placentomegaly
Bone marrow (rare):
“Giant pronormoblasts” with viral inclusions
Considered only in unclear severe anemia cases
Why does Parvovirus B19 cause sudden severe anemia?
B19 selectively infects and destroys erythroid precursors in the bone marrow, stopping red-cell production for 7–10 days.
Why is transient aplastic crisis seen only in patients with chronic hemolytic anemias?
These patients already have rapid RBC turnover; when marrow production stops even briefly, hemoglobin falls dramatically.
Why does the classic “slapped-cheek rash” occur?
Immune-complex deposition in the skin → erythematous malar rash → followed by lacy, reticular rash on limbs.
Why do adults with B19 get arthralgia instead of rash?
Adult immune response favors immune-complex deposition in joints rather than skin, causing symmetric small-joint pain.
Why can Parvovirus B19 infect the fetus but not cause structural malformations?
The virus targets erythroid precursor cells, not organ-forming tissues. Damage occurs by anemia → hydrops, not by teratogenesis.
Why is fetal infection dangerous in the 2nd trimester?
RBC production is maximal; severe anemia → high-output cardiac failure → hydrops fetalis.
Why does Parvovirus not cause chronic hemolysis?
It suppresses erythropoiesis but does not destroy mature RBCs directly; once marrow recovers, anemia resolves.
Why are immunocompromised patients at risk for chronic infection?
They cannot mount adequate neutralizing antibody response → persistent viral replication → chronic pure red-cell aplasia.
Why do some patients show only mild flu-like symptoms?
Host immunity and viral load determine severity; many infections are subclinical.
Why doesn’t Parvovirus B19 commonly cause respiratory symptoms?
Primary infection is viremia-driven; upper airway involvement is minimal compared to viruses like RSV or influenza.
Parvovirus B19 targets erythroid precursor cells in the bone marrow via the P-antigen receptor.
After respiratory entry → virus replicates in the nasopharynx → viremia develops.
Mass destruction of erythroid precursors → transient arrest of erythropoiesis (RBC production stops for 7–10 days).
Immune complex formation (virus + IgM) causes the characteristic “slapped-cheek” rash and arthralgia.
In patients with hemolytic disorders (e.g., thalassemia, sickle cell anemia) → severe anemia occurs due to inability to compensate.
During pregnancy → infection can cause fetal anemia → hydrops fetalis due to high-output cardiac failure.
Virus can persist in immunocompromised hosts → chronic pure red cell aplasia.
Selective tropism for erythroid precursor cells
B19 virus targets pronormoblasts in the bone marrow (via P antigen), causing arrest of erythropoiesis.
Transient red cell aplasia
Destruction of erythroid precursors leads to a drop in reticulocyte count and temporary anemia; severe in patients with hemolytic anemia.
Characteristic “giant pronormoblasts”
Bone marrow shows enlarged pronormoblasts with viral inclusions—pathognomonic.
Immune complex–mediated rash & arthralgia
As viremia declines, IgM and IgG antibodies form complexes → deposition in skin and joints → rash and arthropathy.
Hydrops fetalis pathology
• Fetal anemia → high-output cardiac failure → generalized edema.
• Placental edema and hepatosplenomegaly may be present.
Other tissue effects
• Myocarditis (rare): lymphocytic infiltration of myocardium.
• Vasculitis (rare): immune complex–related vascular involvement.
No vaccine available
There is currently no licensed vaccine for Parvovirus B19.
Good hand hygiene reduces transmission
Frequent handwashing and avoiding touching the face help reduce spread.
Avoid close contact during the viremic phase
Patients are infectious **before the rash appears**. Once rash starts, they are usually no longer contagious.
Pregnancy precautions
Non-immune pregnant women exposed to Parvovirus B19 should undergo IgG/IgM testing and fetal monitoring.
Infection control in schools & healthcare
Routine exclusion after rash is unnecessary, but symptomatic individuals (fever, malaise) should stay home.
Protection of high-risk groups
Immunocompromised patients and those with chronic hemolytic anemia should avoid exposure where possible.
Environmental cleaning
Virus spreads via respiratory secretions; regular cleaning of shared surfaces can help reduce transmission.Dr
Usually normal chest radiograph in erythema infectiosum
Most children have no respiratory involvement, so CXRs are normal.
Bone marrow imaging (rarely required)
• MRI may show diffuse marrow edema during transient aplastic crisis.
• Findings are nonspecific; diagnosis is clinical + laboratory.
Fetal ultrasound (in maternal infection)
Key modality for detecting fetal complications
• Signs of fetal anemia: increased middle cerebral artery (MCA) peak systolic velocity.
• Hydrops fetalis: skin edema, ascites, pleural or pericardial effusion.
• Placental thickening.
Fetal echocardiography
• May reveal high-output cardiac failure due to severe anemia.
Other imaging notes
• No specific CT / MRI findings tied to parvovirus infection in children or adults.
• Imaging is mainly used to evaluate complications such as myocarditis (MRI), or to rule out alternate causes of anemia.
Only one major human pathogenic serotype (B19)
Human parvovirus B19 has a single dominant serotype worldwide, unlike many other viral exanthems.
Genotypes show minor molecular variation
Three main genetic groups are identified: Genotype 1 (most common), Genotype 2, and Genotype 3—but they behave similarly clinically.
No clinically relevant subtype differences
All genotypes produce the same disease spectrum (erythema infectiosum, aplastic crisis, hydrops fetalis), with no difference in severity.
Stable virus with low antigenic drift
Parvovirus B19 undergoes minimal mutation; immunity after infection is typically long-lasting.
*Slapped-cheek erythema* (bright red cheeks with perioral pallor)
Lacy, reticular rash on limbs and trunk
Rash may fluctuate with heat, sunlight, stress
Low-grade fever
Mild cervical lymphadenopathy
Joint swelling/tenderness (adults)
Reduced range of motion due to arthralgia
Pallor (if anemia present)
Tachycardia (in severe anemia)
No significant pharyngitis or conjunctivitis
Helps distinguish from other viral exanthems
Parvovirus B19 causes erythema infectiosum, a mild childhood exanthem characterized by the “slapped-cheek” rash.
It infects erythroid precursor cells → temporary suppression of red-cell production, significant in hemolytic disorders.
Usually self-limiting in children, but can cause aplastic crisis, fetal hydrops, or arthritis in adults.
References
https://imagebank.hematology.org/image/64742/parvovirus-b19-infection-2?type=upload
Dr Sankaran • 2025-11-25 00:31:59
PDF
Bookshelf
Dr Sankaran • 2025-11-25 00:28:43

Bookshelf
Dr Sankaran • 2025-11-25 00:27:50
Bright red “slapped-cheek” rash
Lacy (reticular) rash on arms and trunk
Low-grade fever
Malaise
Headache
Sore throat
Mild arthralgia (children)
*Prominent arthralgia / arthritis in adults* (hands, wrists, knees, ankles)
Fatigue
Low-grade fever
Mild or absent rash (adults)
*Often asymptomatic in pregnancy* (maternal infection)
— but can affect fetus (hydrops fetalis)
Persistent anemia in immunocompromised
Fatigue
Pallor
Minimal or no rash
No specific antiviral therapy required in most cases
Illness is mild and self-limited in immunocompetent children and adults.
Supportive care
Adequate hydration, rest, antipyretics (paracetamol) for fever and discomfort. Avoid NSAIDs in pregnancy unless medically advised.
Arthropathy management
Mild joint pain → paracetamol or short course of NSAIDs (if not contraindicated). Usually resolves spontaneously.
IVIG for immunocompromised with chronic anemia
Intravenous immunoglobulin helps clear persistent infection and corrects red-cell aplasia.
Blood transfusion for severe anemia
Indicated in transient aplastic crisis (e.g., sickle cell disease, thalassemia) with symptomatic or profound anemia.
Fetal management during pregnancy
Weekly ultrasound Doppler monitoring (MCA-PSV) for fetal anemia.
Severe fetal anemia → *intrauterine transfusion* improves survival.
Isolation not required once rash appears
The patient is no longer contagious once the rash starts, so school exclusion is generally unnecessary.
Avoid exposure during pregnancy (preventive advice)
Pregnant contacts should be informed and tested for immunity (IgG).
Tap a card to view full section
Use the coloured cards above (Etiology, Symptoms, Treatment, etc.).